
Author: Dr Laila Surani
A Changing Ageing Landscape
The UK is entering a period of profound demographic change. By 2040, one in four people will be over 65, and an increasing proportion of these older adults will come from minority ethnic backgrounds (Bond, 2025). Migration from South Asia, the Caribbean, Africa, and the Middle East after the Second World War has shaped today’s multicultural Britain. Those who arrived in the 1950s and 1960s are now reaching older age, alongside their UK-born peers.
While diversity has enriched British society, it has also revealed inequalities in ageing. Research consistently shows that older adults from minority groups report poorer health, limited access to services, and higher levels of social isolation compared to White British peers (Age UK, 2022; Watkinson, Sutton & Turner, 2021). The disparities are stark. For example, Bangladeshi and Pakistani elders often experience multiple chronic conditions, while Traveller communities record health outcomes similar to White British individuals twenty years older (Watkinson, Sutton & Turner, 2021).
Where Current Systems Fall Short
National ageing policies are often designed with the idea that a universal model will serve everyone. Yet the lived realities of minority communities do not fit neatly into these frameworks. Some of the recurring gaps include:
Healthcare access: Language difficulties, limited cultural awareness in services, and historical mistrust all hinder engagement (Public Health England, 2018; Alzheimer’s Society, 2021).
Social care: Policy assumes institutional provision is acceptable, but many South Asian and African-Caribbean households expect family-based care, creating tension when traditional models become harder to sustain (Adamson & Donovan, 2005).
Mental health: Depression, dementia, and anxiety are often missed because diagnostic tools overlook cultural differences or because stigma discourages disclosure (NIHR Evidence, 2021).
Economic security: Interrupted employment histories and lower pension entitlements leave many minority elders financially vulnerable (Joseph Rowntree Foundation, 2020).
Housing: Overcrowding and poor housing conditions remain disproportionately high in urban minority populations (Age UK, 2022).
Despite these challenges, minority older people are not passive recipients of care. Community organisations, faith groups, and grassroots initiatives often act as first responders, providing language support, culturally familiar environments, and social contact. However, these organisations remain structurally underfunded and rarely included in national strategies (Centre for Ageing Better, 2020).
Towards a Community-Centred Framework
In reviewing evidence from research, national surveys, and community reports, one message emerges clearly: meaningful solutions must be rooted in communities themselves.
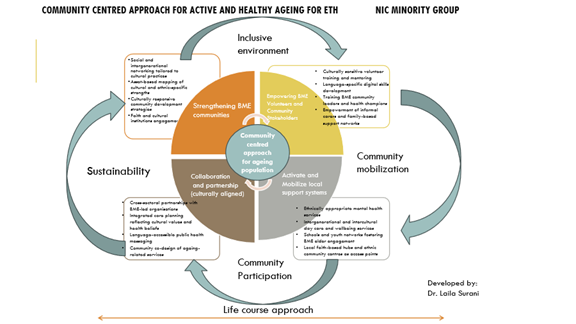
The community-centred framework that I propose builds on four key principles:
1. Cultural competence: Services need to reflect cultural values, languages, and traditions. For instance, incorporating prayer or dietary practices into care settings can help make them more welcoming (Alzheimer’s Society, 2021).
2. Asset-based approaches: Too often, discussions of minority ageing focus on deficits. Yet communities bring rich strengths, including intergenerational support, faith institutions, and cultural traditions that promote resilience (South & Phillips, 2014).
3. Participation and co-production: Older adults from minority backgrounds must have a seat at the table, not only as consultees but as partners in shaping policy and services (NIHR, 2022).
4. Sustainability: Community groups that hold cultural trust require long-term funding and recognition if they are to thrive and continue serving elders effectively.
Four Practical Pillars
Building on these principles, the framework translates into four practical pillars:
–Strengthening communities: Supporting ethnic-specific networks, social clubs, and faith-based initiatives can reduce loneliness and strengthen belonging.
– Empowering volunteers and leaders: Training community champions in digital skills, advocacy, and caregiving helps build capacity from within.
– Mobilising local support systems: Day centres, culturally tailored health services, and intergenerational programmes can bridge gaps left by mainstream services.
– Collaboration and partnerships: Local authorities and statutory bodies must collaborate equitably with BME-led organisations, recognising them as experts in their own right.
This framework is grounded in a life course perspective. Many of the disadvantages faced by older minority adults—such as poor housing, low-paid work, or discrimination in healthcare—are not new but the result of cumulative inequalities across their lifetime (Nazroo, Bécares & Kapadia, 2015).
Looking Beyond the UK
Although this framework arises from UK evidence, it has relevance internationally. The World Health Organization’s Decade of Healthy Ageing (2021–2030) emphasises inclusive environments, integrated care, and equity (WHO, 2021). Other countries have developed creative models that resonate with this approach:
– In Canada, multicultural health brokers bridge linguistic and cultural divides in healthcare.
– In New Zealand, Māori approaches to ageing integrate spirituality, community, and land, demonstrating the importance of indigenous values.
– Across Africa and Asia, extended family networks remain vital for elder care, offering lessons in interdependence and resilience.
These examples show that culturally grounded models are not only possible but essential. The UK can learn from them while also contributing knowledge from its own diverse communities.
Why Action is Urgent
The case for a new framework is pressing.
– Demographic change: With minority groups entering older age in larger numbers, current gaps in provision will soon become unsustainable.
– Economic cost: Poor health and social isolation lead to higher use of crisis services, placing pressure on NHS and social care budgets.
– Social cohesion: Failing to include minority elders undermines trust in public institutions. Conversely, culturally inclusive approaches can foster stronger, more cohesive communities.
If action is delayed, inequalities in later life will deepen, leaving future generations of older adults even more vulnerable.
Policy and Practice Implications
To move forward, several steps are vital:
– Embed co-design with minority elders in local and national policy.
– Invest in community infrastructure, giving grassroots organisations long-term security.
– Train professionals in cultural competence and intersectionality (Bedi & Brown, 2020).
– Reflect faith, family, and intergenerational values in service models.
– Collect and use detailed ethnic data to measure progress transparently.
A Final Reflection
Community-led approaches are not an optional addition to ageing policy; they are a necessity. By centring the voices and strengths of ethnic minority older adults, the UK can create ageing strategies that are inclusive, equitable, and sustainable.
Crucially, what benefits those most marginalised will strengthen the system for everyone. By investing in dignity, cultural recognition, and participation, we can move towards a society where ageing is not marked by inequality but by connection, respect, and opportunity for all.
References
– Age UK. (2022). Later life in the United Kingdom 2022. Age UK.
– Alzheimer’s Society. (2021). Dementia in Black, Asian and minority ethnic communities: The issues. Alzheimer’s Society.
– Bedi, R., & Brown, B. (2020). Intersectionality and cultural competence in health and social care. Routledge.
– Bond, J. (2025). Ageing, diversity, and inequality in the UK. Policy Press.
– Centre for Ageing Better. (2020). The state of ageing in 2020. Centre for Ageing Better.
– Joseph Rowntree Foundation. (2020). Poverty, ethnicity and later life. Joseph Rowntree Foundation.
– Nazroo, J., Bécares, L., & Kapadia, D. (2015). Ethnic inequalities in ageing and health in the UK. Public Health Reviews, 36(1), 1–19.
– NIHR. (2022). Improving inclusion of under-served groups in health research. National Institute for Health Research.
– NIHR Evidence. (2021). Mental health inequalities among minority ethnic communities. NIHR.
– Public Health England. (2018). Health inequalities: Ethnicity and socioeconomic factors. Public Health England.
– South, J., & Phillips, G. (2014). Evaluating community engagement as part of the public health system. Journal of Epidemiology and Community Health, 68(7), 692–696.
– Watkinson, R. E., Sutton, M., & Turner, A. J. (2021). Ethnic inequalities in health-related quality of life among older adults in England: Analysis of the GP Patient Survey. BMJ Open, 11(6), e048290.
– World Health Organization. (2021). Decade of healthy ageing 2021–2030. WHO.